The Safety Culture Gap Behind Healthcare Turnover
Executive summary
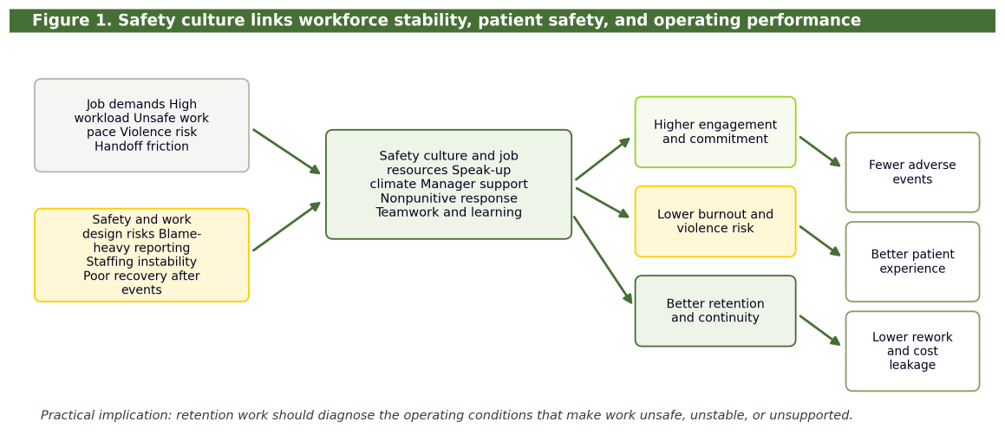
Healthcare organizations do not usually lose good people because they forgot how to recruit. They lose people when daily work starts to feel unsafe, unsupported, and professionally unsustainable. In hospitals and health systems, safety culture is not only a patient safety topic. It is also a workforce stability topic and an operating performance topic. Stronger safety culture is associated with fewer adverse events, lower burnout, lower workplace violence risk, and better conditions for retention (Agency for Healthcare Research and Quality [AHRQ], 2023, 2026; Institute for Healthcare Improvement [IHI], n.d.; Kim et al., 2023; Scott et al., 2022; Vikan et al., 2023; World Health Organization [WHO], 2020). For COOs, CHROs, CNOs, safety leaders, and quality leaders, the practical implication is direct: retention strategy has to include safety culture diagnosis, targeted operational fixes, and a repeatable review cadence.
Safety culture is a retention strategy
Healthcare leaders often separate patient safety, workforce retention, and financial performance into different dashboards. That separation creates blind spots. WHO’s 2020 patient safety campaign made the relationship explicit by framing health worker safety as a prerequisite for patient safety (WHO, 2020). IHI’s National Action Plan also places culture, leadership and governance, workforce safety and well-being, and learning systems in one total-systems framework for safer care (IHI, n.d.).
The healthcare evidence points in the same direction. In a large U.S. academic medical center, better worker-reported patient safety culture was associated with lower odds of workplace violence and lower burnout, with teamwork across units, handoffs and transitions, and staffing playing important roles (Kim et al., 2023). A scoping review found that most studies reported lower adverse-event rates when patient safety culture scores were higher (Vikan et al., 2023). A review of employee engagement and patient safety likewise found a generally positive relationship between engagement and patient safety or quality outcomes, while noting that the strength of the relationship varies by setting, measure, and level of analysis (Scott et al., 2022).
The mechanism is not mysterious. When an organization makes it hard to speak up, hard to hand off safely, hard to recover after adverse events, and hard to work with stable staffing, people do not simply become less engaged. They begin to question whether the work is sustainable. That is when burnout, absenteeism, transfer requests, and resignation become downstream operating indicators (AHRQ, 2023; De Vries et al., 2023; O’Brien et al., 2024).
Why the mechanism matters
The stronger version of the argument draws from two complementary theories. The Job Demands-Resources model explains how physical, emotional, cognitive, and organizational demands deplete people when they exceed available resources. In healthcare, those demands include high workload, unsafe work pace, violence risk, moral distress, poor handoffs, documentation burden, and repeated exposure to adverse events. Resources include manager support, staffing stability, role clarity, team reliability, psychological safety, learning systems, and recovery support (Lopez-Martin & Topa, 2019; Scott et al., 2022).
Social Exchange Theory adds the retention logic. When employees experience visible organizational investment in their safety and well-being, they are more likely to reciprocate with commitment, loyalty, safety behavior, and intent to stay. Evidence from healthcare settings supports this pathway. Aman-Ullah et al. (2022) found that workplace safety related to employee retention through job satisfaction and employee loyalty among physicians. Sam-Mensah et al. (2025), in a non-healthcare public-sector sample, similarly found that safety and health rules and organizational safety support were linked to lower turnover intentions through organizational commitment. These findings should be applied cautiously across contexts, but they reinforce the same practical point: safety investments become retention investments when employees experience them as real support, not as compliance messaging.
Workplace violence makes the link more urgent
Workplace violence should not be treated as a separate security issue. It is part of safety culture, work design, patient experience, and retention. Arnetz (2022) notes that workplace violence threatens health worker safety and well-being, productivity, retention, and quality of care. The Joint Commission’s workplace violence prevention standards, implemented in 2022, require accredited hospitals to address worksite analysis, data monitoring, staff education and training, and leadership accountability for prevention programs (Arnetz, 2022).
O’Brien et al. (2024) describe workplace violence as a growing burden shaped by patient and family distress, long waits, communication problems, crowding, behavioral health needs, unmet expectations, and resourcing failures. That means prevention cannot rely only on de-escalation training. Leaders also need to examine throughput, access, staffing, triage workflows, security response, communication protocols, and post-event support. When employees believe violence is simply part of the job, organizations lose both incident data and trust.
What leaders should measure
AHRQ’s SOPS Hospital Survey 2.0 gives leaders a strong starting point. Its core domains include teamwork, staffing and work pace, organizational learning/continuous improvement, response to error, supervisor and manager support for patient safety, communication about error, communication openness, event reporting, hospital management support, and handoffs or information exchange (AHRQ, 2026). Those domains should not sit alone in a quality department report. They should be linked to workforce and operational stability signals.
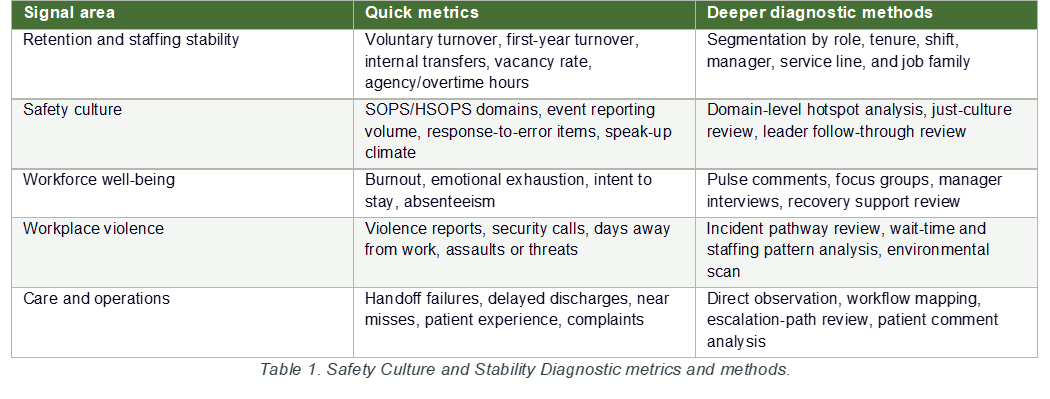
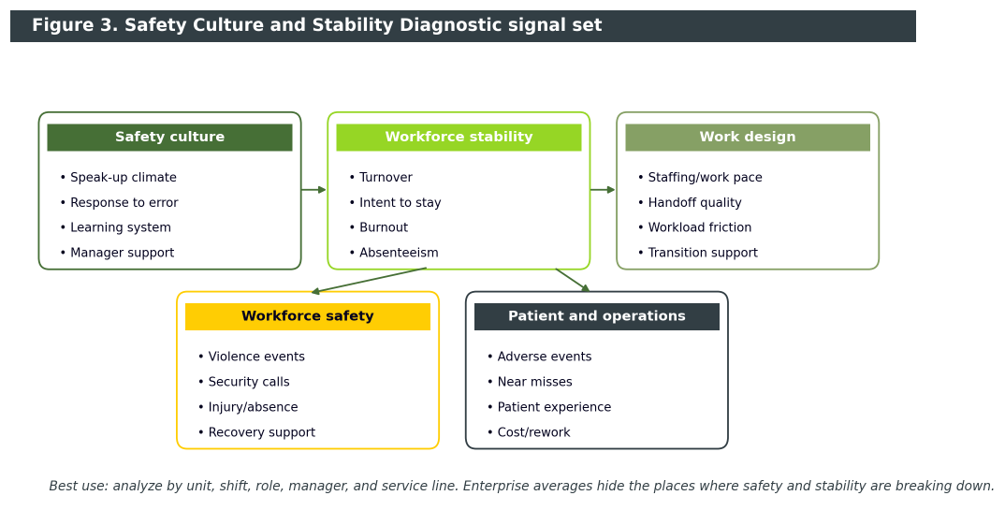
For senior leaders, the most useful view is unit- or service-line level, not only enterprise level. Enterprise averages hide hotspots. The priority signals are safety culture survey domains, voluntary turnover, first-year turnover, internal transfers, vacancy rate, agency use, overtime, intent to stay, emotional exhaustion, absenteeism, staffing stability and work pace, handoff quality, workplace violence, event reporting volume, response-to-error patterns, and patient experience, especially communication and coordination (AHRQ, 2026; Kim et al., 2023; Scott et al., 2022).
What actually improves retention when safety culture is weak
The first intervention is leadership behavior. A culture of safety is built when leaders make it safe to report hazards, respond visibly to concerns, avoid blaming individuals for system failures, and close the loop after issues are raised. AHRQ’s PSNet emphasizes that adverse events are rarely isolated individual failings. Organizations need system fixes, transparent reporting, and support for affected workers after adverse events (AHRQ, 2023).
The second intervention is staffing and continuity repair. Kim et al. (2023) found that staffing, teamwork across units, and handoffs or transitions were major predictors of workplace violence and burnout. Retention work should therefore include schedule stability, vacancy management discipline, safer throughput, standardized handoffs, stronger escalation routines, better onboarding, and preceptor support for new staff.
The third intervention is workflow redesign. De Vries et al. (2023) found that many retention interventions cluster around onboarding, transitions to new units, stress coping, social support, extra staffing, work organization, and mentoring. Hoxha et al. (2024) also highlight the role of organizational culture, supportive environments, recognition, development opportunities, and process improvement in job satisfaction and healthcare quality. The practical point is that resilience training cannot substitute for fixing the work.
The fourth intervention is reinforcement. Recognition is useful when it reinforces the behaviors that make care safer: speaking up, safe handoffs, timely escalation, team backup, patient-centered problem solving, and manager follow-through. Organizations often recognize volume and heroics. They should also recognize prevention, reliability, and learning.
How I help leaders solve the problem
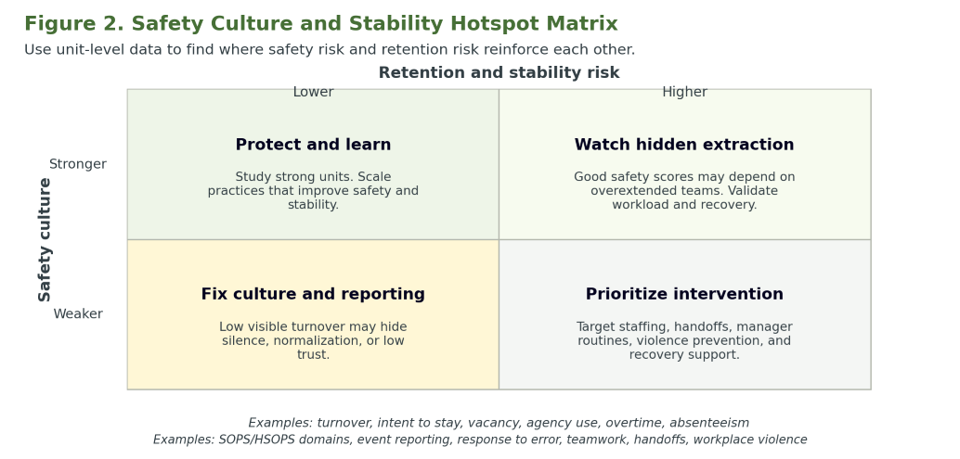
My consulting approach starts with diagnosis. The Safety Culture and Stability Diagnostic links SOPS/HSOPS culture domains with turnover, intent to stay, burnout, staffing stability, handoff quality, workplace violence, patient experience, and operating indicators. The goal is not another generic culture presentation. The goal is to identify the units where weak culture and unstable work design are driving retention risk.
The second step is prioritization. Rather than launching an enterprise-wide campaign, I help leadership focus on the services where risk, cost, and strategic importance intersect. The third step is targeted intervention. Depending on the diagnostic results, that may include manager routines, just-culture strengthening, handoff redesign, onboarding or preceptor redesign, schedule stability work, violence-prevention workflow changes, or post-event recovery support. The fourth step is sustainment: monthly unit reviews, quarterly executive reviews, and annual culture assessment with pulse work between full survey administrations (AHRQ, 2026; De Vries et al., 2023; IHI, n.d.).
Common pitfalls
The most common leadership error is using pay as the only retention lever. Compensation matters, but the evidence points to a broader operating system: safety, support, mentoring, workload, culture, and work organization all shape intent to stay (De Vries et al., 2023; Williams & Beidas, 2018). The second error is treating safety culture as a survey rather than a management system. The third is trying to coach resilience while leaving staffing, handoffs, workflow, and violence risk unchanged. The fourth is tolerating blame-heavy reporting environments, which discourages speaking up and accelerates disengagement (AHRQ, 2023).
Evidence-quality note
The directional evidence is strong enough for action, but leaders should avoid oversimplifying it. Several studies are cross-sectional, some use self-reported outcomes, and some safety-retention evidence comes from non-U.S. or non-hospital settings. The best practical conclusion is not that any single score perfectly predicts turnover. The stronger conclusion is that patient safety culture, workforce safety, engagement, burnout, and retention are linked closely enough that leaders should diagnose and manage them together rather than separately (Scott et al., 2022; Vikan et al., 2023).
Safety Culture and Stability Diagnostic
If your organization is trying to improve retention without diagnosing safety culture, it is probably treating symptoms rather than causes. The Safety Culture and Stability Diagnostic gives leaders a practical way to identify where culture, staffing, workflow, workplace violence, and retention risk are colliding, and where leadership action will have the greatest impact first. Download the Diagnostic Summary.
References
Agency for Healthcare Research and Quality. (2023, March 21). Impact of system failures on healthcare workers. PSNet. https://psnet.ahrq.gov/
Agency for Healthcare Research and Quality. (2026). SOPS® Hospital Survey. U.S. Department of Health and Human Services. https://www.ahrq.gov/sops/surveys/hospital/index.html
Aman-Ullah, A., Ibrahim, H., Aziz, A., & Mehmood, W. (2022). Impact of workplace safety on employee retention using sequential mediation: Evidence from the health-care sector. RAUSP Management Journal, 57(2), 182-198. https://doi.org/10.1108/RAUSP-02-2021-0043
Arnetz, J. E. (2022). The Joint Commission’s new and revised workplace violence prevention standards for hospitals: A major step forward toward improved quality and safety. The Joint Commission Journal on Quality and Patient Safety, 48(5), 241-245. https://doi.org/10.1016/j.jcjq.2022.02.001
Arzahan, I. S. N., Ismail, Z., & Yasin, S. M. (2022). Safety culture, safety climate, and safety performance in healthcare facilities: A systematic review. Safety Science, 147, Article 105624. https://doi.org/10.1016/j.ssci.2021.105624
De Vries, N., Lavreysen, O., Boone, A., Bouman, J., Szemik, S., Baranski, K., Godderis, L., & De Winter, P. (2023). Retaining healthcare workers: A systematic review of strategies for sustaining power in the workplace. Healthcare, 11(13), Article 1887. https://doi.org/10.3390/healthcare11131887
Hoxha, G., Simeli, I., Theocharis, D., Vasileiou, A., & Tsekouropoulos, G. (2024). Sustainable healthcare quality and job satisfaction through organizational culture: Approaches and outcomes. Sustainability, 16(9), Article 3603. https://doi.org/10.3390/su16093603
Institute for Healthcare Improvement. (n.d.). Safer together: A national action plan to advance patient safety. https://www.ihi.org/
Kim, S., Kitzmiller, R., Baernholdt, M., Lynn, M. R., & Jones, C. B. (2023). Patient safety culture: The impact on workplace violence and health worker burnout. Workplace Health & Safety, 71(2), 78-88. https://doi.org/10.1177/21650799221129264
Lopez-Martin, E., & Topa, G. (2019). Organizational culture and job demands and resources: Their impact on employees’ wellbeing in a multivariate multilevel model. International Journal of Environmental Research and Public Health, 16(17), Article 3006. https://doi.org/10.3390/ijerph16173006
O’Brien, C. J., van Zundert, A. A. J., & Barach, P. R. (2024). The growing burden of workplace violence against healthcare workers: Trends in prevalence, risk factors, consequences, and prevention. eClinicalMedicine, 72, Article 102641. https://doi.org/10.1016/j.eclinm.2024.102641
Sam-Mensah, R., Bingab, B. B. B., Boakye, K. O., & Boateng, R. K. (2025). Safety first, retention forever: Enhancing commitment and reducing turnover through safety practices. Future Business Journal, 11, Article 52. https://doi.org/10.1186/s43093-025-00475-0
Scott, G., Hogden, A., Taylor, R., & Mauldon, E. (2022). Exploring the impact of employee engagement and patient safety. International Journal for Quality in Health Care, 34(3), Article mzac059. https://doi.org/10.1093/intqhc/mzac059
Vikan, M., Haugen, A. S., Bjørnnes, A. K., Valeberg, B. T., Deilkås, E. C. T., & Danielsen, S. O. (2023). The association between patient safety culture and adverse events: A scoping review. BMC Health Services Research, 23, Article 300. https://doi.org/10.1186/s12913-023-09332-8
Williams, N. J., & Beidas, R. S. (2018). Navigating the storm: How proficient organizational culture promotes clinician retention in the shift to evidence-based practice. PLOS ONE, 13(12), Article e0209745. https://doi.org/10.1371/journal.pone.0209745
World Health Organization. (2020). World Patient Safety Day 2020: Health worker safety: A priority for patient safety. https://www.who.int/